




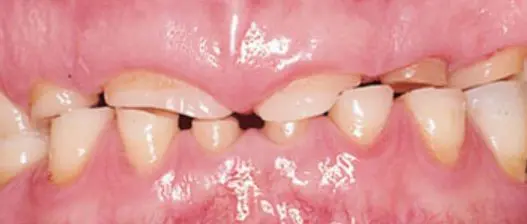

If the tooth structure loss is severe then the treatment is usually some kind of dental restorations. Depends on the case, this can be done with composite restorations, metal restorations, removable partial dentures or dental crowns and bridges. The decision to restore the damaged teeth depends on the wants and needs of the patient, the progression of tooth surface loss and whether tooth surface loss is active or inactive.
Our Location
Call Us
Send a Mail
Working hours
9-6 PM Monday to Saturday
