Endodontic Therapy or Root Canal Treatment (RCT) is necessary procedure for diseases related to infection of dental pulp tissue or periapical tissue. When caries occurs and it is not stopped in the early stage, the infection progresses deeper to the dental pulp. Dental pulp is tissue that fills the canal system in the centre of the tooth, containing mostly nerves, vascular tissue and immune cells. When bacteria from caries arrive in dental pulp, different scenarios are possible, depending on the patient’s immunity status and bacterial flora. These different pathological changes have different approaches to treatment, but what is common for all of them, they all request adequate endodontic treatment.
{kind=link}
The infection of pulp can have acute or chronic pathology, with or without pus and with a different clinical presentation. Acute pulpitis is usually followed by spontaneous, pulsating pain that increases during the night and the pulp tissue is partially or entirely inflamed. After removing the inflamed tissue from dental chamber and canals, complete endodontic treatment can be performed in a single visit. On the other hand, chronic pulpitis may persist as asymptomatic or may become symptomatic when acute exacerbation occurs with symptoms similar to an acute form of this condition. There are many other forms of chronic pulpitis like epulis, where granulation tissues overgrow the dental chamber and dental crown. If pulpitis stays untreated it can progress to pulp necrosis or periodontitis. Pulpal necrosis is the consequence of chronic pulpitis that may have clinical painful manifestation or may stay unnoticed and accidentally discovered during teeth examination.
Depending on clinical manifestation, initial diagnoses and patient’s chief complaints, therapy may begin with first aid treatment that includes tooth trepanation in order to achieve a proper drainage of inflamed tissue. In some cases surgical incision of surrounding tissue may be necessary, followed by antibiotic medication. Acute conditions require the reduction of pain and after the acute inflammatory phase is under control it can proceed with endodontic treatment in order to exclude bacteria from the tooth’s canals and periapical tissue.
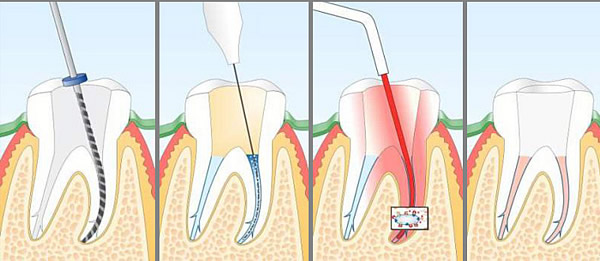
After opening the tooth, whether as a drainages opening of regular access to the tooth’s canal system, the right preparation of dental chamber is necessary. This stage is called access cavity preparation and has the aim of forming the ideal entrance for endodontic instruments into the canal system. There should be no obstacles for the instruments so the canal preparation can be achieved with minimal mechanical resistance to the instruments. There are many types of endodontic instruments from many different companies. These instruments are formed as needles, made of curved wire by special technological processes, with sharp edges that allow mechanical clearance of dental canal’s walls. The most known are K shaping files, reamers and tapers.
After the access cavity is properly prepared, the first step is the determination of the working length. With proper files known as progliders or pathfinders, the initial scouting and passability of canal system are required. With a help of additional equipment called Apex Locator, the length of each canal may be precisely determined. Canal length is the distance from the referent marked point on the tooth’s crown and tooth’s apex. The precise length is one of the major measures that affect the outcome of endodontic treatment.
In some cases, mostly in periodontitis with huge bone destruction and pus collection, intersession treatment and medication may be necessary in order to more effectively destroy all pathogen bacteria. Intersession medication includes the application of sterile calcium-hydroxide or sometimes even antibiotic paste known as Trio-paste.
When instrumentation and medication of canals are finished, whether it is performed through one or more sessions and after proper final irrigation, canals should be dried and properly obturated. There are few different techniques for canal obturation: lateral condensation, vertical compaction, cone-fit technique. They all have the same purpose, to tightly close the empty space of the canals in there full diameter and length.
After endodontic treatment is finished, depending on the tooth’s crown condition, your dentist will suggest the best solution for final crown restoration. Whether it includes core build-up with additional composite filling, onlay or overlay, or maybe a dental crown. Final crown restoration is equally important as proper endodontic treatment since coronal sealing is of major importance in preserving the treated canals from repeated bacterial penetration.
It is important to understand the significance of endodontic therapy. This procedure allows the tooth preservation for long period of time, even when only the root has left. A financial calculation can easily justify the price of these complex procedures since they are cheaper than tooth loss and consequential implant placement. There is no superior substitute for our natural tissue and nothing is more valuable than our own natural teeth.